Our previous blog noted the patellofemoral joint (PFJ) could be a major source of anterior knee pain following ACL reconstruction (ACLR), given the high prevalence of PFJ and tibiofemoral joint (TFJ) joint changes as early at 12 months (Culvenor et al., 2015)
This month we are reviewing who may be at risk of early joint changes (PFJ/TFJ).
What factors may predict future OA post ACLR?
- Patellofemoral cartilage lesion at time of injury (Li et al., 2012)
- Previous history of patellofemoral pain (Utting et al, 2005)
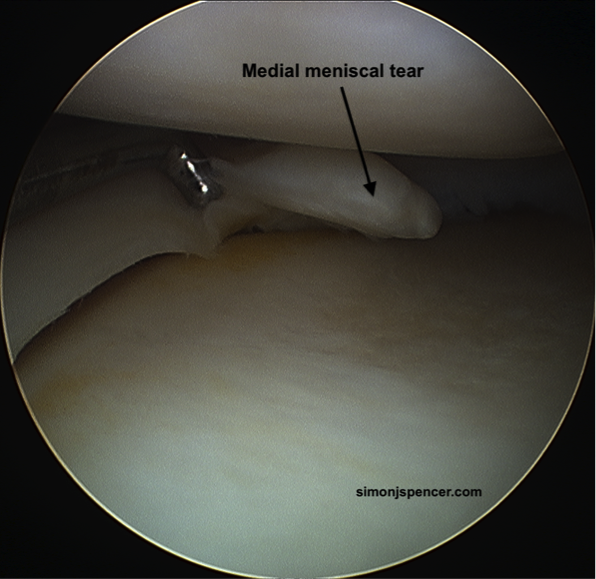
- Previous menisectomy (Li et al., 2012)
- Menisectomy at time of surgery (Culvenor et al., 2015)
- Crepitus (Schipof et al., 2014)
There is limited evidence on modifiable risk factors such as strength and function and their predictive relationship with future joint health/OA:
- Pincewski et al., 2007 showed < 90% single hop test at 1 year predicted > radiographic OA at 10 years.
- BMI >25 at time of surgery (Culvenor et al., 2015)
Some cross sectional studies suggest an association of OA with altered biomechanics (at a particular time point post ACLR):
– Altered gait biomechanics (< KF in stance, increased tibial ER, compared to hea lthy) associated with greater amounts of OA (Culvenor et al., 2014, Hart et al., 2015)
lthy) associated with greater amounts of OA (Culvenor et al., 2014, Hart et al., 2015)
– Altered landing biomechanics (<KF compared to healthy) associated with greater amounts of PFJ OA.
However, more prospective studies are required to determine whether these alterations existed prior to injury, or are consequences of the injury/surgery/ongoing neuromuscular deficits.
Will they be symptomatic?
- At 12 months post ACLR there was no association between PFJ OA (MRI defined) and pain/symptoms (Culvenor et al., 2015)
- However, we know that this population presents with poor outcomes in follow ups > 12 months (symptoms, function, quality of life) AND
- There are links between poor patient reported outcomes and physical testing performance (6-12 months post ACLR)
- These include; < 22 on one leg rise, <88% on single and triple cross over hop for distance, < 90% quadriceps strength) (Culvenor et al., 2016, Pincewski et al., 2007, Logerstedt et al., 2012, Pietrosome et al., 2016)
Take home messages:
- Joint changes are present and progress early post ACLR. Patients may or may not be symptomatic.
- Identification of risk factors may assist clinicians in being wary of knee joint loading, progression and education of those who may fall into these categories.
- Modifiable risk factors should be addressed
E.g. Targeted movement retraining to improve sagittal plane kinematics in gait and landing tasks.
E.g. Full restoration (>95%) of strength and functional testing, (? >100% if dominant leg)