
- Exercise after cancer is associated with a reduction in cancer related death by up to 50%.
- Exercise may also reduce the risk of cancer recurrence by up to 35%.
- Exercise is the number one treatment for the most common and debilitating side effects of cancer – cancer related fatigue.
- Exercise is also helpful in remedying numerous other treatment side effects including reducing depression, preventing lymphedema and improving fitness and strength.
- There is also emerging data that exercise during toxic cancer treatments can improve the effectiveness and completion rates of chemotherapy.
Yet, for the estimated 400,000 cancer survivors in Australia, most will not have access to critical exercise based rehabilitation programs.
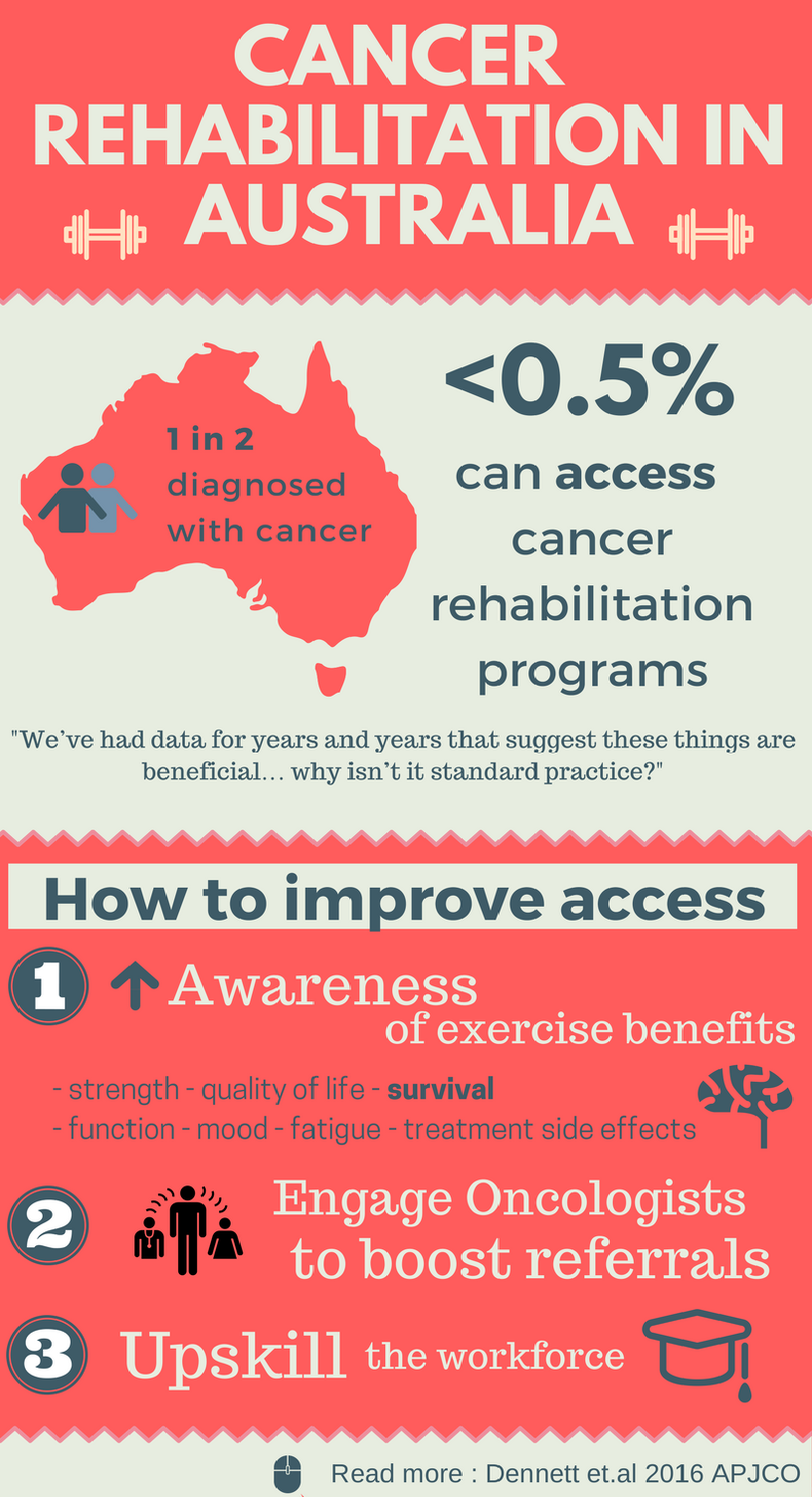
It is currently not routine practice to cancer survivors to be referred to rehabilitation. Our nation first review of cancer rehabilitation practices identified only 31 cancer specific rehabilitation programs exist in Australia, enough to service just 0.5% of cancer survivors. Unfortunately, we are not alone, with a lack of provision in cancer rehabilitation worldwide. This is problematic given cancer survivors report high levels of unmet needs, with 60% expressing need for rehabilitation. Furthermore, one study has identified as little as 2% of survivors reporting physical impairment will be referred for ongoing care.
How we can increase access to cancer rehabilitation services?
1. Increase awareness about the benefits of exercise during cancer recovery. The concept of exercising with cancer is relatively new. Only 20 years ago, it was thought that exercise was unsafe for people to exercise with cancer through fears it would exacerbate fatigue or make the cancer worse and these ideas continue to exist today. In fact, the opposite is true. Increasingly, patients that are aware of the benefits indeed do want to exercise. Most would be on board if they were to have a recommendation from their oncologist.
2. Identify what models of cancer rehabilitation work best. The ideal model of cancer rehabilitation hasn’t been established. A number of rehab models exist including prospective surveillance and the cardiac rehabilitation model of care. We still don’t know what is most effective and therefore, it’s harder to integrate cancer rehabilitation into health systems. Research shows that among people with heart disease, cardiac rehabilitation programs reduces death by up to 26%. We now need this same hard data showing cause and effect for cancer rehabilitation. Good news is two large international studies are underway in an attempt show this– the CHALLENGE TRIAL for people with colon cancer and the INTERVAL trial for men with prostate cancer.
3. Upskill the workforce to train professionals in this complex area. Work is currently underway with the Australian Physiotherapy Association to develop a career pathway for physiotherapists working in cancer care.
4. Implement policy so rehabilitation can be recognised as STANDARD cancer care. By making referrals for exercise rehabilitation routine, we can reduce barriers to rehabilitation so we can improve the quality (and maybe even quantity) of the lives of those affected by cancer.